This page is provided for patients with diabetes using insulin who would like to improve their control by being proactive instead of reactive to their test results.
Traditionally patients tested their glucose and used an "insulin sliding scale" (ISS) to determine how much insulin they should then take. This is a reactive and retrospective response to a pre-meal glucose level largely determined by previous food intake and the insulin covering that intake. It may have very little relevance to the insulin needed to cover the next meal.
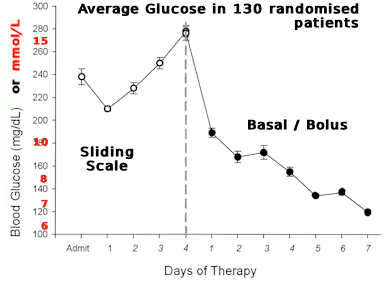
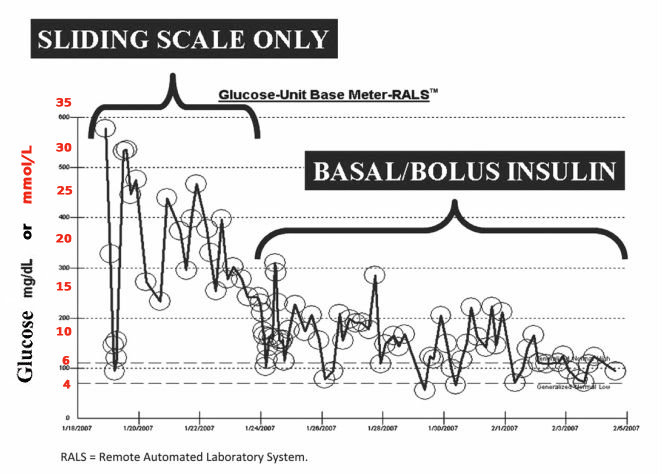
The use of ISS to manage diabetes is a common practice in hospitals as well as long term care facilities Ref 1. These are dosing schedules that guide insulin administrators (e.g. nurse practitioner or patient) to inject insulin based on blood glucose readings. Again, this means a ISS treats hyperglycaemia after it has occurred, making ISS a�"reactive" approach. Many studies have shown �that using ISS alone to manage diabetes is an ineffective way to manage blood glucose levels Ref 1. In fact, traditional ISS leads to what is known as the "Roller Coaster" effect, as seen in the image on the left. Instead, guidelines and evidence advocate for a�"proactive" approach�to managing blood glucose levels, using basal and bolus insulin as seen in the image on the right.
"Reactive" Approach
- "Reactive" Insulin Treatment = Insulin Sliding Scale (ISS) Ref 1;
- Treating hyperglycaemia after it has already occurred (Too Late!);
- Involves adjusting dose of insulin based on a single blood glucose
reading;
- Leads to a "Roller Coaster" effect, exacerbating hyperglycaemia
as well
as hypoglycaemia (as seen in the image below) Ref 2
|
|
"Proactive" Approach
- "Proactive" approach= Basal-bolus insulin regimen (BBI);
- Anticipates changes in blood glucose and prevents them from occurring Ref 1;
- Insulin regimen is adjusted based on blood sugar patterns over the
past few days-weeks;
- Mimics physiological release of insulin Ref 1
|
 Ref 3
Ref 3
Above is the effect of a ISS approach....
|
|
Ref 2
The above image is an example of a patient switched from traditional insulin sliding scale (ISS) to basal-bolus insulin (BBI) regimen. When the patient was on the traditional ISS, the they had large glycemic variabiltiy (the "roller coaster" effect). By switching to a BBI regimen, one can see a clear reduction in glucose fluctuations as well success in achieving and maintaining the ideal range.
|
|
Both the average and the example graphs above show the effect of changing from an ISS regime to a BBI regime with a basal dose of the 24hr acting glargine (Lantus) (50% of total) combined with three
pre-meal bolus doses of rapid acting glulisine (Apidra) (the other 50%), subsequently adjusting the basal insulin according to fasting glucose and the pre-meal Apidra bolus according to it's previous effect.
The average graph on the left shows a significant difference ("P" value of < 0.05).
|
| |
|
This essentially means that in order to improve diabetic control one needs to stop reacting and start being pro-active.
For instance for a patient on "basal" Lantus (long acting) and "bolus" Apidra (rapid acting)....
- The dose of Lantus should be adjusted up or down if the fasting (eg pre-breakfast) glucose level is consistently high or low (respectively) as those results best reflect the basal glucose levels.
- The dose of the pre-breakfast Apidra should be adjusted up or down based on what previous AFTER usual breakfast glucose levels (known as 2 hour post-prandial [=2h pp] levels) were, not any before breakfast test (as those reflect the basal glucose managed by the basal Lantus dose).
- Similarly, the dose of the pre-lunch Apidra should be adjusted up or down based on what previous AFTER usual lunch glucose levels (2h pp levels) were, not any before lunch test (as those reflect the effect of the pre-breakfast Apidra, the breakfast and post-breakfast activity it covered).
- Likewise, the dose of the pre-dinner/tea Apidra should be adjusted up or down based on what previous AFTER usual dinner/tea glucose levels (2h pp levels) were, not any before dinner test (as those reflect the effect of the pre-lunch Apidra, the lunch and post-lunch activity it covered).
- Finally, if the fasting morning test is higher than the after dinner test, one could be experiencing hypoglycaemia (low glucose) during the night resulting in adrenalin and cortisol release which results in higher glucose levels, known as the Somogyi rebound effect. This can be confirmed by doing a middle of night test showing a low glucose (one may need to set an alarm). Manage by either having a supper before bed or if trying not to gain weight, reduce the before dinner Apidra (or possibly reduce the basal Lantus a bit).
Overall, one needs to look at patterns of glucose 2 hours AFTER the rapid acting insulin has been given and the meal taken. Except for the pre-breakfast test (which best measures basal glucose), any before meal tests are just confirmation that the glucose has returned to normal after the previous meal and unless wildly raised should not influence the decision about how much insulin is needed for the following meal. To see patterns best it is helpful to graph results by time of day in a logbook such as the CareSens Log Book or use the Smartlog Desktop or phone ap (where one should view the Daily Trend overlay graph). Looking at a number of days' 2h pp results at a particular time helps decisions about whether more of less insulin is needed in the future given before that type of meal.
During illness, fasting glucose levels can indicate if the Lantus dose should be increased. Note that illness normally increases insulin requirements but this can change quickly so more frequent testing and watching trends is even more important.
Dr Keith Blayney
|
References:
- Guillermo E. Umpierrez, Dawn Smiley, Ariel Zisman, Luz M. Prieto, Andres Palacio, Miguel Ceron, Alvaro Puig and Roberto Mejia "Randomized Study of Basal-Bolus Insulin Therapy in the Inpatient Management of Patients With Type 2 Diabetes (RABBIT 2 Trial)"�Diabetes Care 2007 Sep; 30 (9): 2181-2186. https://doi.org/10.2337/dc07-0295
- Schmeltz, LR "Management of Inpatient Hyperglycemia" Lab Medicine (Oxford Academic) 2011; 42(7): 427-434
Lowell R. Schmeltz, MD, Management of Inpatient Hyperglycemia, Laboratory Medicine, Volume 42, Issue 7, July 2011, Pages 427�434 https://doi.org/10.1309/LMU72V7QWUDUYQIJ
- Eradicating Insulin Sliding Scales : Resource Guide for Pharmacists https://eliminateinsulinslidingscale.weebly.com/
|
|