Obesity Therapy (weight loss treatments)
Go directly to Intuitive Eating
Having faced some weight issues myself, I have watched the research and response to treatments over the last 40+ years and witnessed outcomes (good and bad). I can offer the following advice:
[A] Measurement
The standard Total Weight or even Body Mass Index (weight in Kilograms divided by height squared in Metres [Kg/m²]) have serious shortfalls as they don't differentiate between fat, muscle, organs, bones and water. As such it over-estimates risk for those who are fit and well muscled (like many All Blacks), Polynesians and water retaining individuals, while under-estimating risks for anorexics, elderly (especially those with osteoporosis) and unfit individuals. Furthermore, weight loss may be hidden for those who combine exercise with diet, as muscle weighs more than fat so the scales may show no obvious improvement and as such disincentivise their lifestyle changes.
Body fat percentge is a more accurate estimate of health risk but is harder to measure. It can be estimated from:
- Skin fold caliper measurements using various calculators (an option at our surgery);
- Calculators using gender, age, height, weight, neck and waist measurements (eg body-fat-calculator based on a US Navy method).
- Hydrostatic Weighing; Air Displacement Plethysmography; Bioelectrical Impedance etc and
- Various scans such as DEXA and MRI.
Waist measurement, by far the simplest measurement available to individuals to accurately monitor response to obesity management (and reduced risk). There are three simple ways to do this:
- Tape measure: Measure on skin (not over clothes), infront of a mirror (to ensure tape is horizontal), held firmly but not tight, placed immediately above umbilicus (belly button) and after exhaling. In general men should aim to get below 94cm and women below 80cm. This is the simplest single measure but the significance is affected by ethnicity.
- Waist to Height Ratio: Take as in (1.) but also measure height (in bare feet), using the same system (centimetres or in inches) but don't tell me in inches, (or for that matter use pounds and ounces for babies) - unless you want to be reminded that I haven't used imperial measures since 1967, and it is as confusing as using Fahrenheit for temperature!
Where were we, oh yes, the goal is to get below 50% (Girth to Height).- Clothes size: You know you are winning when you can fit those jeans that shrunk after having children!
[B] Weight Loss Medication
Until recently no anti-obesity drug worked particularly well, and every one that led to even modest weight loss had serious side effects.
Some of those "serious" side effects included deaths, heart attacks, strokes, pulmonary fibrosis, pancreatitis and dependence, while other side effects were more just inconvenient like faecal incontinence (Xenical), insomina and anxiety, but all medicines were not funded and only worked while being taken (so needing long term cost, as well as risk) with weight returning when they were stopped. The most effective were combinations like naltrexone/bupropion (Contrave) and the most effective phentermine/topiramate (not available as a combination in NZ). The usual reasoning of "to kick off the weight loss" was just not supported by the evidence.More recently we have seen diabetes medications that reduce both stomach emptying and appetite called Glucagon-like peptide-1 receptor (GLP-1 for short) agonists (Dulaglutide = Trulicity and Semaglutide = Ozempic (not available in NZ) or Wegovy) and analogues (Liraglutide = Victoza or Saxenda) used to produce significant weight loss. Liraglutide is a daily injection which can produce 5 -10kg weight loss without the apparent risks but is expensive (approx $550 per month) while semaglutide is a weekly injection and only available as Wegovy and probably "only" $500 per month. Studies reveal an average 15kg weight loss. Trulicity and Victoza are only available for diabetics in NZ as supplies ran out with non-diabetic use. Duaglutide (Trulicity) gives a modest weight loss in about a third of diabetic patients.
Side effects of GLP-1 agonists include dry mouth, low glucose, malnutrtion, facial aging and bowel problems including a life-threatening pulmonary aspiration anesthesic risk if patients are unable to stop 3 weeks prior to surgery - see Note 2. Weight loss on GLP-1 agonists includes muscle and bone mass but weight gain after stopping is mainly fat so people may well end up fatter and less healthy, as well as poorer!
Those intending to use a GLP-1 agonist for weight loss are encouraged by endocrinologists to see an endocrinologist - see Note 3./
Those "put off" by cost, side effect and rebound issues of medication are better to look at "Phenotype Guided" approaches, initially designed to help select best weight reducing medications but can equally be applied to selecting the most appropriate behavioural changes. There is good evidence that this approach is far more effective as everyone has different causes and drivers and we now have a evidence based and easily understood "pathophysiology classification of Obesity Phenotypes".
[C] Diet and exercise
- Traditionally diet and exercise have been largely unsuccessfully "prescribed" to patients to lose weight. Formal Weight Watchers and Jenny Craig programs have been successful but weight gain tends to "relapse" when people go back to their previous habits. Regular aerobic exercise (including the use of a "Green Prescription") also works for many until the exercise habit ends.
- Weight reducing exercise doesn't have to be strenuous or prolonged like marathons, mountain climbs or 30km bike rides. Recent evidence shows that "short, sharp" (High Intensity Interval Training) exercise; low impact, resistance, relaxing, stretching (yoga, Palates, Tai Chi and even planking) exercise; and just building exercise into your normal day (not parking too close to destination, biking to work, getting up between clients, using stairs not lift/escalator) can be just as effective.
- In weight management programs, 90% of those who maintained their weight loss for five years exercise an hour each day.
- Very Low Calorie diets (eg Optifast) combined with the threat of "no surgery until you achieve a 10% weight loss" are highly effective prior to surgery but are not sustainable or healthy, but of course they are not needed after bariatric surgery.
- Dietitians can have more success as they look at your usual diet (so take a food diary to your appointment) and may suggest achievable modifications (so not massive changes that are unlikely to be sustained). Remember all Dietitians are nutritionists but only nutritionists with a nationally recognised undergraduate science degree in human nutrition, as well as a Masters Degree or Postgraduate Diploma in Dietetics can be registered as a dietitians, meaning you can trust a dietitian to give credible evidence-based advice. Anyone can be a nutritionist.
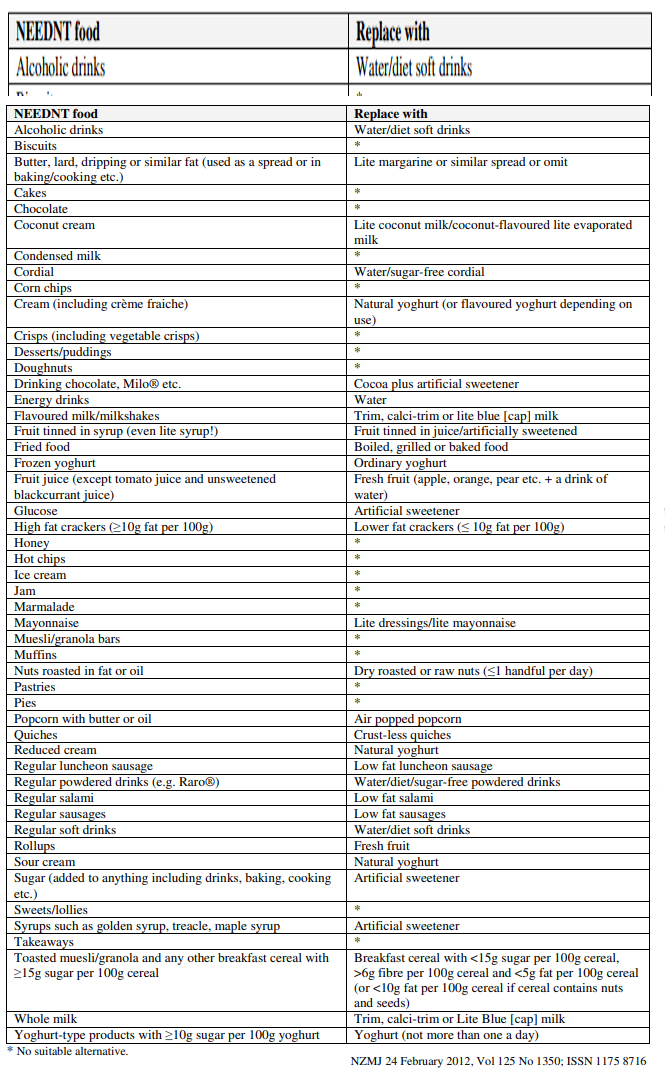
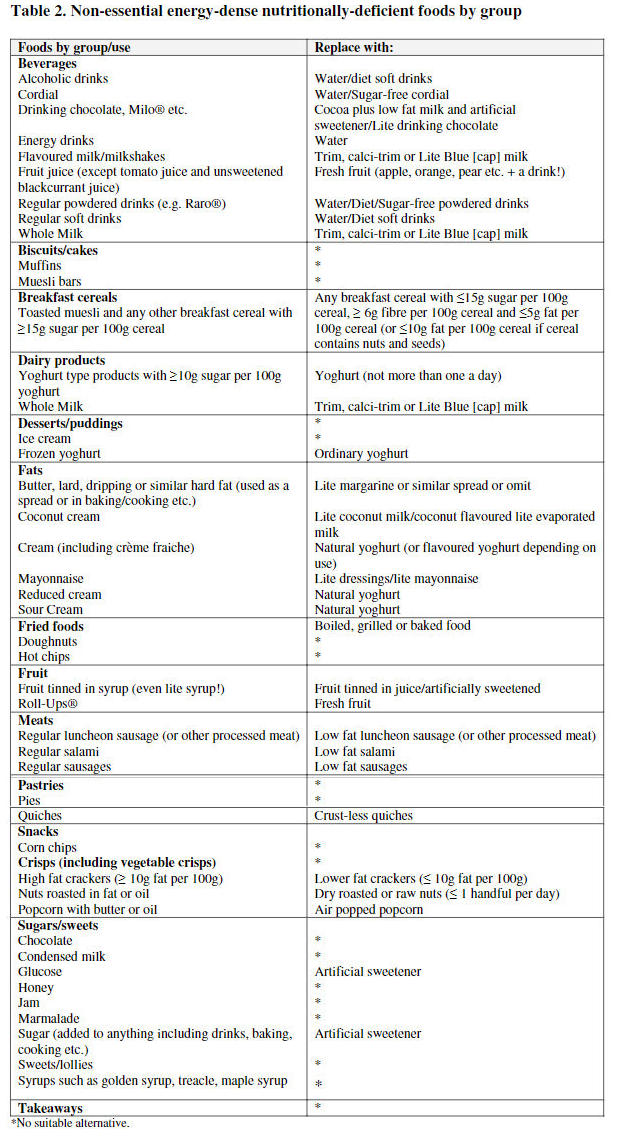
- Identify foods that are non-essential, energy dense and/or nutritionally deficient (NEEDNT) and find alternatives that have lower calories and/or are more nutritious. A NEEDNT food alphabetical list or NEEDNT food category list, with alternative choices was compiled from the National Heart Foundation, Diabetes New Zealand and CDHB lists in 2012 and published in the New Zealand Medical Journal for all to see. See Note 4
- Many people opt to miss meals hoping this will reduce totally calories consumed, but does this work? The answer is very clear from repeated studies that it depends on which meal. I often find patients unable to loose weight report regularly missing breakfast and the studies show for the same daily calories, avoiding eating after dark results in twice the weight loss (up to 10% of BMI) compared to missing breakfast Note 14. On the other hand there is no strong evidence to support the idea that eating breakfast aids weight loss Note 15, consistent with the Intuitive approach. Dietitians note that not all breakfasts are equal and those high in refined carbohydrates and low in fiber and protein tend to increase subsequent hunger and are associated with poor diabetic control while breakfasts rich in fiber, protein, and healthy fats can help people feel full for longer. Most concerning of all was a 2019 review of available studies that revealed people who regularly skipped breakfast were about 21% more likely than regular breakfast consumers to experience a cardiovascular "incident" and had a 32% higher all-cause death risk Note 16.
- Self-generated strategies such as smaller sized plates, fruit as "between meal snacks", intermittent fasting, reducing processed carbs, removing obvious fat, only eating when hungry, following a diabetic diet etc can all be useful adjuncts.
- There is however clear evidence that to sustain weight loss with whatever diet and/or exercise combo you elect, you need strategies that sustain successful lifestyle changes - see Psychology.
[D] Bariatric Surgery
Bariatric (weight loss) surgery is done usually when diet and exercise haven't worked or when you have serious health problems because of your weight. The surgery is considered successful if you lose 50% of your excess weight and keep it off. By this standard, the success rate for Bariatric Surgery is 90%. Weight loss is mostly long-term but some regain up to 25% after two years.
Side effects (other than surgical complications of bleeding, infection, clots (DVT, PE), obstruction, leaks and death) include Dumping Syndrom (nausea, sometimes with associated low glucose levels); malabsorption; bile reflux, gallstones and depending on amount of weight loss, loose skin folds.
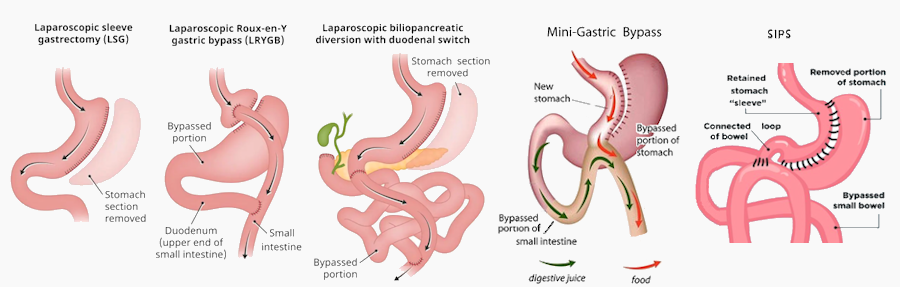
Types of bariatric surgery:
- Gastric sleeve - becoming the most common mainly because it is a relatively simple procedure with little risk of complications. It removes about 80% of the stomach leaving a small tubular portion (the sleeve). This reduces the quantity of food eaten and produces a full feeling.
- Gastric bypass aka "Roux-en-Y" - the stomach is divided to create a small pouch which limits how much can be eaten and empties into the middle of the small intestine.
- Mini Gastric bypass aka Laparascopic "Single Anastomosis Gastric Bypass" (SAGB) is a simpler variant of the Roux-en-Y - with a long, narrow gastric pouch which is joined to the small bowel, bypassing 1.5 to 2 meters of the small 'bowel giving few complications but excellent results (75% weight loss at one year). This is also becoming very popular.
- Biliopancreatic diversion with duodenal switch (BPD-DS) - combines a sleeve gastrectomy with an intestinal bypass, similar but more extreme than a "Roux-en-Y". This also limits how much you can eat and reduces the absorption of nutrients. While it is extremely effective, it also has greater risk, including malnutrition and vitamin deficiencies.
- Stomach Intestinal Pylorus Sparing Surgery (SIPS) aka Loop Duodenal Switch or SADI-s - a modified version of the original duodenal switch with only one anastomosis and less small bowel bypassed i.e. intended to reduce complications.
- Stomach Stapling - verticle banded gastroplasty has largely been abandoned because of poor results.
- Stomach Banding - placing an adjustable band at the upper part of the stomach to reduce hunger but unfortunately it is less effective than bypass and sleeve procedures and there is concern about a high late complication rate.
Bariatric surgery costs between $25,000 - $30,000 privately in New Zealand and only a limited number of people aged between 18 and 60 years are eligible for publicly funded weight loss surgery. Criteria includes having a BMI of 40 or more or a BMI of 35 or higher and other obesity-related severe diseases that could be improved by surgery and have previously failed attempts to lose weight. However only 400 are done each year in the public system with a national rate of 2.7 per 1,000 morbidly obese (ranging from less than 0.5/1,000 in MidCounties to 8.8/1,000 in Waitemata [See Note 5]. Some health insurance companies can help.
[E] Psychological approaches
There are a number of psychological concepts that affect the success or not of weight loss. We have concepts such as:
- "Some people have an 'all or nothing' attitude and think about weight loss in terms of being 'on' or 'off' a diet. Psychologists work with people to address negative feelings and find ways to reward healthy changes to their eating habits."
- "Most people start their weight-loss journey feeling like losing the weight is going to be the hardest part. When they lose weight, they feel successful. But eventually they go right back to their old habits."
- "Emotional and restrained eating styles have been found to be related to negative psychological and physical health outcomes (including weight gain)....intuitive eating is positively related to psychological and physical health outcomes." See Intuitive eating
- "The key to maintaining weight loss is making a range of behavioral and lifestyle changes to counteract deeply ingrained, lifelong habits....If it was just a hunger thing, we'd eat when we are hungry and stop when we're full....it takes even more practice to maintain weight loss, because you have to maintain a healthy lifestyle."
So essentially we need mechanisms to maintain the healthy lifestyle changes, to avoid slipping back into old habits. Traditional "psychological" mechanisms like "get more sleep" and "reduce stress" (with yoga, meditation, mindfulness, exercise etc.) are aspirational concepts, but not always practical and some lack a good evidence base. Stress is an individual response that can be modified (either by adapting / problem-solving or acceptance, depending on whether the stressor is modifiable or not), which is better than just masking our response with the traditional approaches.
Outcomes (like achieving and maintaining weight loss) need to use some evidence based psychological tools of behaviour change like diversion (thought blocking), new habit developement and reinforcement (rewards).Possible strategies include:
- Divert negative self-talk (thought blocking): Instead of blasting yourself with criticism or discouragement ("I've blown it, I'll never keep the weight off"), redirect your thoughts to positive ones like "my next treat will be some healthy fruit - put that on the shopping list". There are on-line Cognitive Behaviour sites or better still seeing a Cognitive Behaviour Therapist that can be helpful in training this important tool.
- Keep healthy snacks available: Have apples, nuts or other good snacks at home (instead of biscuits, cakes and chocolate) and stocking your work space similarly allows you to bypass the pastries etc without having to find that mythical "willpower".
- Similarly the fridge can contain some healthy options like chilled lemon water, iced tea, low fat yoghurt for when we stray there.
- Plan alternatives to "comfort food" so one can easily choose non-food-related rewards such as listening to music, reading a book, taking a stroll or shopping.
- Plan your meals: Decide in advance what you're going to cook, then shop for and limit yourself to those choices.
- Use mind tricks like using smaller, dark-colored (eg blue) plates and bowls, to make the food more obvious and larger appearing; increase fibrous-rich vegetables to increase satiation; healthy snacks between meals reduces binge eating.
- Use "Mindfulness in eating" techniques. See Mindfulness Eating
- Intuitive Eating - a modern highly effective strategy - Eat tasty food when you're hungry and stop when you're no longer hungry. This means giving yourself permission to stop eating when hunger is abolished (don't wait until you feel full or the plate is empty). It is, however, important to inform the partner who may have prepared the food to avoid the impression you don't like their cooking!
To make this work one needs to break old habits of "saving the best until last" and "eat what's on your plate". Replace these with new habits of "eat the best bits first" as this not only makes your new habit rewarding, it makes it easier to leave the less nutritious calorie dense carbs/starch and fatty bits.
Two further benefits of this approach are: [1] over the following hours there is only one real source for extra energy needs (fat stores), so this drives weight loss and [2] if you want a desert or snack later, it isn't adding to excess calories, it is providing what you need. Formal studies are showing this approach is highly successful in weight reduction and maintenance of that reduction - see Notes 6-7.- Be accountable - keep exercise logs, food diaries and regular "same time of the day" waist measures (I recommend avoiding scales as the muscle weight you gain may mask the fat loss). Mark the hole in the belt where you feel comfortable so you are aware if the beltline is shrinking or not. This feedback reinforces successful behaviour and identifies unhelpful patterns, particularly looking for trends over time.
- Make exercise rewarding - time spent walking with partner or friend, family outing to climb a hill, use that smart watch to monitor speed, distance etc, join a group (Pilates, Tai chi, Karate) and do fun activities like low setting reps on circuit training, cycling somewhere new.....
- Reinforce success with non-food but relevant rewards such as buying that smaller size clothing item you now fit, doing that bush walk you couldn't manage before, making another hole in a belt for your next goal, buy some nice walking shoes etc
Finally, while the "Intuitive eating" approach is better for self-esteem and weight loss than "Restrained eating", it is also compatible with outcome based Cognitive Behavior Therapy (CBT). CBT fits with changing unhealthy "restrictive" concepts and behaviours to those that work and improve mental and emotional health. The underlying assumptions of behavioral and CBT treatments are that behaviours can be learned, unlearned, modified, and replaced by other behaviours through different strategies, some of which include goal setting, problem solving, stimulus control and self-monitoring. Recent reviews (meta-analysis of randomized trials) have shown the efficacy of CBT in weight loss (of 8-10%) Note 8-11, including maintenance of weight loss, particularly when provided by professionals and multidisciplinary teams Note 12. Self-help CBT or interventions by nurses with limited CBT training alone were less effective Note 13.
According to the American Psychological Association, CBT, in general, is based on these core principles:
CBT can help change harmful behavioral patterns including:
- Psychological problems are based, in part, on faulty or unhelpful ways of thinking.
- Psychological problems are based, in part, on learned patterns of unhelpful behavior.
- People suffering from psychological problems can learn better ways of coping with them, thereby relieving their symptoms and becoming more effective in their lives.
- over-eating
- sedentary lifestyle
- reactions to stress
[F] Obesity Phenotypes used to guide weight loss options
In 2021 the US Mayo Clinic performed randomised trials targeting therapy to phenotype-guided or non-phenotype (patient and/or physician preference) and demonstrated a significant outcome difference with 79% of the phenotype-guided group losing over 10% weight compared to 34% in the non-guided group Note 17, Note 18. While the trials looked at types of medication, they identified and defined four major obesity phenotypes that non-pharmacological, especially psychological approaches, can be more accurately applied.
The phenotypes can even be specifically tested for (if not obvious). They Are:
- Hungry Brain (poor satiation) [32%]
The brain-gut axis mis-matching calories to satiety (not knowing when the meal is over)
Test: ab libitum buffet meal consuming more kcal (p<0.001)
Targeted lifestyle advice / options:
- Time restricted eating (Mayo Clinic)
- Hi-fibre and coloured, unpeeled vegetables, whole unprocessed food (increasing satiation feeling)
- Intuitive eating (evidence based)
Hungry Gut (poor satiety) [32%]
Reduced ability to not eat between meals
Test: Much faster gastric emptying (p<0.001)
Targeted lifestyle advice / options:
- Low Cal. diet with pre-meal protein supplements (Mayo Clinic)
- Hi-fibre, high protein diet eg legumes
- 30 min supine (on back) after meals
Emotional Hunger (hedonic eating) [21%]
A desire to eat to cope with positive or negative emotions
Test: Much higher HADS (Hospital Anxiety and Depression Score) (p<0.001)
Targeted lifestyle advice / options:
- Low Cal. diet plus Group Therapy (Mayo Clinic)
- "Safer" food available (eg fruit) with no biscuits/cakes/chocolate etc to tempt
- Individual Cognitive Behaviour Therapy Note 19, Note 20
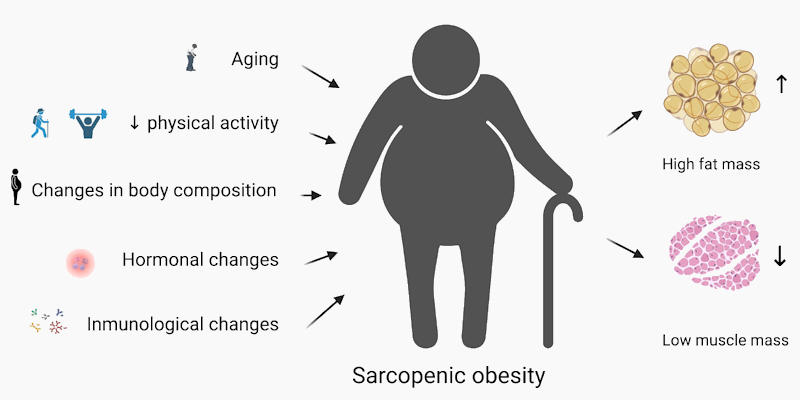
Slow Burn (reduced metabolic rate) [21%]
Typical of sarcopenic obesity in older, less active people.
Test: Much lower REE (Resting Energy Expenditure) (p<0.001) and self-reported exercise
Targeted lifestyle advice / options:
- Low Cal. diet plus Group Therapy (Mayo Clinic)
- High intensity interval training with post workout protein supplementation (Mayo Clinic)
- "Safer" food available (eg fruit) with no biscuits/cakes/chocolate etc to tempt
- Check thyroid function and sleep duration (>9hr a risk) Note 21,
- Resistance or Mixed training reduces body fat but not weight (muscle weighs more!) Note 22
- Only whey protein supplementation has neen shown to be effective Note 23,
15% of obesity patients don't fit any phenotype group, while 27% actually fit more than one group, so those people could try strategies from each of the groups that they fit. Trying to address or adapt to the pathological process driving an individual's obesity is not just logical but more likely to achieve sustained improvement.
[G] References[Compiled by Dr K T Blayney]
- US Navy based Body Fat Calculator https://www.calculator.net/body-fat-calculator.html.
- Canadian Journal of Anesthesia paper body-fat-calculator; https://link.springer.com/article/10.1007/s12630-023-02550-y#author-information.
- David Kim, Auckland endocrinologist https://cardiologyinstitute.co.nz/gp-info/2023/5/16/glp-1-agonists-faq.
- Elmslie, J. L. et al; The NEEDNT Food LIST: non-essential, energy dense, nutritionally deficient foods The New Zealand Medical Journal 24 February 2012, Vol 125 No 1350; ISSN 1175 8716 https://assets-global.website-files.com/5e332a62c703f653182faf47/5e332a62c703f671382fdf20_elmslie.pdf).
- Associate Professor Dr Rinki Murphy (University of Auckland) https://www.auckland.ac.nz/en/news/2019/04/15/postcode-lottery-for-weight-loss-surgery.html#:~:text=They%20found%20that%20of%20approximately,per%201000%20in%20MidCentral%20and).
- Markey, C. H., Strodl, E., Aimé, A., McCabe, M., Rodgers, R., Sicilia, A., Coco, G. L., Dion, J., Mellor, D., Pietrabissa, G., Gullo, S., Granero-Gallegos, A., Probst, M., Maïano, C., Bégin, C., Alcaraz-Ibáñez, M., Blackburn, M-E, Caltabiano, M. L., Manzoni, G. M. ... Fuller-Tyszkiewicz, M. (2023). A survey of eating styles in eight countries: Examining restrained, emotional, intuitive eating and their correlates. British Journal of Health Psychology, vol. 28, Issue 1, pages 136-155 February 2023. https://bpspsychub.onlinelibrary.wiley.com/doi/10.1111/bjhp.12616.
- Taylor, Victoria What is intuitive eating? Heart Matters Magazine, British Heart Foundation https://www.bhf.org.uk/informationsupport/heart-matters-magazine/nutrition/weight/intuitive-eating.
- Foster, G. D., Makris, A. P. & Bailer, B. A. Behavioral treatment of obesity 1-4. Am. J. Clin. Nutr. 82, 230-235 (2005) https://www.sciencedirect.com/science/article/pii/S0002916523295386?via%3Dihub.
- Jacob, A. et al. Impact of cognitive-behavioral interventions on weight loss and psychological outcomes: A meta-analysis. Health Psychol. 37, 417-432 (2018) https://psycnet.apa.org/doiLanding?doi=10.1037%2Fhea0000576.
- Mesarič, K., Pajek, J., Logar Zakrašek, B. et al. Cognitive behavioral therapy for lifestyle changes in patients with obesity and type 2 diabetes: a systematic review and meta-analysis. Sci Rep 13, 12793 (2023).
https://doi.org/10.1038/s41598-023-40141-5.- ComÛa, L., David, O. & David, D. Outcomes and mechanisms of change in cognitive-behavioral interventions for weight loss: A meta-analysis of randomized clinical trials. Behav. Ther. Res. https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijn.12690.
- Fernández-Ruiz, V. E. et al. Short-medium-long-term efficacy of interdisciplinary intervention against overweight and obesity: Randomized controlled clinical trial. Int. J. Nurs. Pract. 24(6), e12690 (2018). https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijn.12690.
- Madjd, A. et al. Effects of cognitive behavioral therapy on weight maintenance after successful weight loss in women; a randomized clinical trial. Eur. J. Clin. Nutr. 74, 436-444 (2020). https://www.nature.com/articles/s41430-019-0495-9.
- Kelly, Kevin Parsons et al. Eating breakfast and avoiding late-evening snacking sustains lipid oxidation. PLOS Journal, February 27, 2020. https://doi.org/10.1371/journal.pbio.3000622.
- Sievert, Katherine et al Effect of breakfast on weight and energy intake: systematic review and meta-analysis of randomised controlled trials BMJ 2019;364:l42 https://www.bmj.com/content/364/bmj.l42.
- Ofori-Asenso R, Owen AJ, Liew D. Skipping Breakfast and the Risk of Cardiovascular Disease and Death: A Systematic Review of Prospective Cohort Studies in Primary Prevention Settings. J Cardiovasc Dev Dis. 2019 Aug 22;6(3):30. doi: 10.3390/jcdd6030030. PMID: 31443394; PMCID: PMC6787634. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6787634/.
- Andres Acosta, Michael Camilleri, Barham Abu Dayyeh, Gerardo Calderon, Daniel Gonzalez, Alison McRae, William Rossini, Sneha Singh, Duane Burton, Matthew M. Clark "Selection of Antiobesity Medications Based on Phenotypes Enhances Weight Loss: A Pragmatic Trial in an Obesity Clinic Obesity (Silver Spring). 2021 Apr;29(4):662-671. doi: 10.1002/oby.23120. Erratum in: Obesity (Silver Spring). 2021 Sep;29(9):1565-1566. doi: 10.1002/oby.23236. Erratum in: Obesity (Silver Spring). 2022 Jul;30(7):1521. doi: 10.1002/oby.23498. PMID: 33759389; PMCID: PMC8168710. https://onlinelibrary.wiley.com/doi/10.1002/oby.23120.
- Acosta A, Camilleri M, Abu Dayyeh B, Calderon G, Gonzalez D, McRae A, Rossini W, Singh S, Burton D, Clark MM. "Selection of Antiobesity Medications Based on Phenotypes Enhances Weight Loss: A Pragmatic Trial in an Obesity Clinic. Obesity (Silver Spring)". 2021 Apr;29(4):662-671. doi: 10.1002/oby.23120. Erratum in: Obesity (Silver Spring). 2021 Sep;29(9):1565-1566. doi: 10.1002/oby.23236. Erratum in: Obesity (Silver Spring). 2022 Jul;30(7):1521. doi: 10.1002/oby.23498. PMID: 33759389; PMCID: PMC8168710. https://pubmed.ncbi.nlm.nih.gov/33759389/.
- "Emotional Eating and Obesity: An Update and New Insights" https://link.springer.com/article/10.1007/s13679-025-00661-9?utm_source=getftr&utm_medium=getftr&utm_campaign=getftr_pilot&getft_integrator=wiley .
- Thomas A. Wadden, Gary D. Foster "BEHAVIORAL TREATMENT OF OBESITY, Medical Clinics of North America, Volume 84, Issue 2, 2000, Pages 441-461, ISSN 0025-7125, doi.org/10.1016/S0025-7125(05)70230-3 or www.sciencedirect.com/science/article/pii/S0025712505702303
- Yang M, Zhang Y, Zhao WY, Ge ML, Sun XL, Jia SL, Dong BR. Association of sleep duration with sarcopenic obesity in multi-ethnic older adults: findings from the WCHAT Study. BMC Geriatr. 2022 Nov 24;22(1):899. doi: 10.1186/s12877-022-03543-0. PMID: 36434541; PMCID: PMC9701023. https://pmc.ncbi.nlm.nih.gov/articles/PMC9701023/
- Chen, L., Zhou, H., Gong, Y. et al. "Clinical outcome changes in sarcopenic obesity: a meta-analysis of exercise training methods." BMC Geriatr 25, 33 (2025). doi.org/10.1186/s12877-024-05655-1
- Cheah KJ, Cheah LJ. "Benefits and side effects of protein supplementation and exercise in sarcopenic obesity: A scoping review." Nutr J. 2023 Oct 23;22(1):52. doi: 10.1186/s12937-023-00880-7. PMID: 37872544; pmc.ncbi.nlm.nih.gov/articles/PMC10591413/
[]



{kind=link}
{kind=link}
{kind=link}